Hernias and Peritoneal Dialysis
If you were to think of your abdominal wall, you might picture a solid sheet of muscle. That's just what you should have to keep your bowel where it belongs. But sometimes there is a chink in your muscle armor—a small tear that can let the inner lining of your abdomen push through. This tear is a hernia. Hernias can occur more often if you do peritoneal dialysis (PD).
Types of hernias
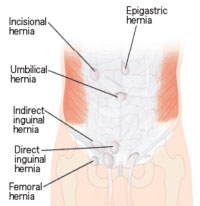
There are four main types of hernia that are more likely to occur on PD: 1
- Direct or indirect inguinal hernia
- groin
- Exit site hernia
- where the catheter comes out of your body
- Umbilical hernia
- belly button
- Incisional hernia
- any other spot where you have had surgery on your abdomen
When you do PD, umbilical and inguinal hernias are the most common types.
What to watch for
You can often see the bulge of a hernia. An umbilical hernia looks as if an "innie" belly button has become an "outie." Call your doctor if you notice any new bumps or bulges in your belly. An inguinal hernia will bulge down into the groin, where you can feel it, but may not be able to see it.
Having a hernia can cause pain while lifting, or a dull ache. On PD, two hernia problems can also become serious:
- A loop of bowel is caught
- A hernia is "strangulated" when part of the bowel comes through the hole and is trapped. If the blood supply is cut off to the bowel, gangrene can occur. This is a life-threatening emergency—and a good reason to have a hernia fixed sooner rather than later.
- PD fluid leaks out
- Having PD fluid in your belly raises the pressure in your abdomen. Plus, extra fluid is present that can leak out. With a hernia, PD fluid may leak at the catheter exit site. Or, in men, an inguinal hernia that leaks due to the pressure of PD fluid in the belly can lead to painful swelling of the scrotum. Special X-ray imaging can help find this problem.
Hernia risk factors
 Anyone can have one or more hernias. In fact, 73% of hernias in people on PD occur
before
the start of treatment.
2
Any surgery to your abdomen can leave a weak spot that may be more prone to a hernia down the road. Other factors have also been linked to a higher risk of hernia—whether or not you are on PD. These include:
Anyone can have one or more hernias. In fact, 73% of hernias in people on PD occur
before
the start of treatment.
2
Any surgery to your abdomen can leave a weak spot that may be more prone to a hernia down the road. Other factors have also been linked to a higher risk of hernia—whether or not you are on PD. These include:
- Being male 3
- Being born with an abdominal wall with weak spots (more likely if your mother was very young when she had you) 4
- Having autosomal dominant polycystic kidney disease 5
- Being overweight 5
If you have any of these risk factors and have not started PD, ask your doctor to check for hernias so they can be fixed first.
On PD, you can reduce your risk of a hernia if you avoid things that increase pressure in your abdomen, like:
- Constipation
- Constant coughing 6
- Heavy lifting or jumping
- Higher-volume PD fills 7
- Not getting enough PD 3
Hernia repair: What to expect
The good news is, hernias can be fixed. If you are on PD—or want to start—there are a number of good options for you.
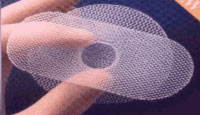
Hernia repair on PD works best if a strong, sterile surgical mesh is used to close the tear in the muscle wall. In one 4-year study, 12% of hernias that were fixed without the mesh came back. None of the mesh repaired hernias did. 8
 General anesthesia is used for a hernia repair. The surgeon may use a laparoscope to see inside your belly, or may do an open repair, with a larger incision. A very large hernia might mean you will have a drain tube. You may be in the hospital for 4 to 10 days, based on how the surgery is done.
General anesthesia is used for a hernia repair. The surgeon may use a laparoscope to see inside your belly, or may do an open repair, with a larger incision. A very large hernia might mean you will have a drain tube. You may be in the hospital for 4 to 10 days, based on how the surgery is done.
Afterward, you'll have pain pills to take. You'll need to keep your stitches dry. And, you'll be asked not to drive or to lift anything heavy (over 10 lbs.) for 4-6 weeks.
If you have not yet begun PD and have a hernia, a surgeon may be able to fix it and place a PD catheter at the same time. This has been done with inguinal hernias9, and may be possible with other types as well. (Avoid having a PD catheter placed in the mid-line of your belly, which may be weaker than the sides.)
Doing PD after a hernia repair
Once on PD, you may worry that having a hernia fixed means you must use standard in-center hemodialysis until you are healed. Not true! One option after surgery is to use low-volume, recumbent-only (LVRO) PD. 10 This means using smaller fills and only doing exchanges while you lie down to reduce the pressure in your abdomen.
Another option is to do an exchange the day of the surgery, no dialysis for 48 hours, then slowly restart PD. In one study, patients did CAPD 3 days a week (10 hours) for 2 weeks, then smaller fills for 2 weeks, and were back to the normal prescription by 4 weeks. On a cycler, exchanges were done 3 days a week for one week, then every other night for 4 weeks. None of the 50 patients had a leak, and none of their hernias came back early due to the PD. 11
No one wants to have a hernia, but today the chances are good that having one will not keep you from doing PD.
References:
- Abdominal hernias in continuous peritoneal dialysis
- Garcia-Urena MA, Rodriguez CR, Vega Ruiz V, Carnero Fernandez FJ, Fernandez-Ruiz E, Vazquez Gallego JM, Velasco Garcia M. Prevalence and management of hernias in peritoneal dialysis patients. Perit Dial Int. 2006 Mar-Apr;26(2):178-82
- Van Dijk CM, Ledesma SG, Teitelbaum I. Patient characteristics associated with defects of the peritoneal cavity boundary. Perit Dial Int. 2005 Jul-Aug;25(4):367-73
- Castilla EE, Mastroiacovo P, Orioli IM. Gastroschisis: International epidemiology and public health perspectives. Am J Genet C Semin Med Genet. 2008 Aug 15;148C(3):162-79
- Del Peso G, Bajo MA, Costero O, Hevia C, Gil F, Diaz C, Aguiera A, Selgas R. Risk factors for abdominal wall complications in peritoneal dialysis patients. Perit Dial Int. 2003 May-Jun;23(3):249-54
- Cobb WS, Burns JM, Kercher KW, Matthews BD, James Norton H, Todd Heniford B. Normal intraabdominal pressure in healthy adults. J Surg Res. 2005 Sep 1
- Dejardin A, Robert A, Goffin E. Intraperitoneal pressure in PD patients: relationship to intraperitoneal volume and PD-related complications. Nephrol Dial Transplant. 2007. May;22(5):1437-44
- Martinez-Mier G, Garcia-Almazan E, Reyes-Devesa HE, Garcia-Garcia V, Cano-Gutierrez S, Mora Y, Fermin R, Estrada-Oros J, Budar-Fernandez LF, Avila-Pardo SF, Mendez-Machado GF. Abdominal wall hernias in end-stage renal disease patients on peritoneal dialysis. Perit Dial Int. 2008 Jul-Aug;28(4):391-6
- Singh CA, Singh NS, Moirangthem GS, Singh TS, Singh KL, Singh LR, Sharma LR, Mebang M. Simultaneous continuous ambulatory peritoneal dialysis catheter implantation and inguinal hernia repair. J Indian Med Assoc. 2006 Mar;104(3):122-3, 128
- Tast C, Kuhlmann U, Stolzing H, Alscher D, Mettang T. Continuing CAPD after herniotomy. EDTNA ERCA J. 2002 Oct-Dec; 28(4): 173-5M.
- Shah H, Chu M, Bargman JM. Perioperative management of peritoneal dialysis patients undergoing hernia surgery without the use of interim hemodialysis. Perit Dial Int. 2006 Nov-Dec;26(6):684-7